| dc.contributor.advisor | Jakola, Asgeir Store | |
| dc.contributor.author | Sjåvik, Kristin | |
| dc.date.accessioned | 2018-06-06T13:04:31Z | |
| dc.date.available | 2018-06-06T13:04:31Z | |
| dc.date.issued | 2018-06-08 | |
| dc.description.abstract | Abstract
Background
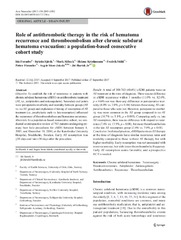
Perioperative treatment for common neurosurgical conditions such as chronic subdural hematomas (CSDH) and meningiomas vary. The perioperative period is by definition the time span from 24 hours before surgery until 30 days postoperatively. Even if the surgical treatment in the operation theater can be exactly the same, complication rates differ, and results vary. The aim of the thesis was to compare recurrences after CSDH burr-hole surgery using three different drainage techniques, to establish the risk of recurrence in CSDH patients using antithrombotic (AT) medication, to clarify the risk/benefit ratio of prophylactic pharmacotherapy initiated the evening before craniotomy for meningioma, and to identify important predictors for complications in meningioma surgery. A future more large-scale aim was to clarify whether this pragmatic research design could be used for further quality work in practical neurosurgery.
Methods
A comparative effectiveness framework was created to conduct retrospective reviews in different Scandinavian cohorts from three different neurosurgical departments (Karolinska University Hospital, University Hospital of North Norway and St. Olavs University Hospital). The Scandinavian cohorts were all population-based, and all patients treated between 2005 and 2013. Studies included large number of patients ranging from 763 to 1260 patients.
Results
Active subgaleal drainage for 24 hours after surgery seems to be the most efficient and safest treatment strategy for chronic subdural hematoma. Patients with CSDH on antithrombotic therapy at the time of diagnosis, have similar recurrence rates and mortality compared to those without antithrombotic therapy. Early AT resumption is not associated with more recurrence, but with lower thromboembolic frequency. As needed perioperative administration of low molecular weight heparin, reserved for patients with excess risk because of delayed mobilization, is effective and appears to be the safest strategy, rather than routine administration. Severe complications after meningioma resection are more encountered in elderly patients (>70 years old), dependent patients (Karnofsky performance scale <70), and patients who undergo longer lasting surgery (>4 hours). Patient selection, including careful consideration of the individual risk-benefit ratio, is important in improving the safety of intracranial meningioma resection.
Conclusion
The framework with its population-based studies provided valid results for the clinical questions raised. The researchers will continue to work on establishing evidence-based guidelines for common neurosurgical conditions within the established research platform. | en_US |
| dc.description.doctoraltype | ph.d. | en_US |
| dc.description.popularabstract | Tunge kirurgiske fag baserer mye av virksomheten på tradisjoner og gammel overtro. Den nye generasjonen kirurger vil ha forskningsbasert, strømlinjeformet behandling av ypperste klasse.
Nevrokirurgi, eller hjernekirurgi om du vil, er et fag forbundet med høy risiko. Selv om operasjonene stort sett gjøres på samme måte enten du får behandling i Tromsø, København eller Stockholm, varierer komplikasjonsratene ved denne type inngrep betydelig.
Tre ulike nevrokirurgiske avdelinger i Skandinavia har gått sammen om prosjektet ”Perioperativ kvalitetssikring i nevrokirurgi”. Med hovedforankring i Tromsø har man gått systematisk gjennom forløpet ved mer enn 2000 hjerneoperasjoner, og allerede endret viktige faktorer som er avgjørende for hvordan det går med pasientene.
For et relativt lite sykehus som UNN er det viktig å dokumentere at vi leverer behandling av høy kvalitet. Det gjør vi, og det har vi nå igjen solide tall på. Fagmiljøet i Skandinavia har tatt imot de nye forskningsresultatene med åpne armer. | en_US |
| dc.description | Paper I of this thesis is not available in Munin:<br>Assessment of drainage techniques for evacuation of chronic subdural hematoma: a consecutive population-based comparative cohort study. Sjåvik K., Bartek J., Sagberg, L.M., Henriksen, M.L., Gulati, S., Ståhl, F.L., Kristiansson, H., Solheim, O., Förander, P., Jakola, A.S. Available in <a href=http://dx.doi.org/10.3171/2016.12.JNS161713>Journal of Neurosurgery. 2017 Jun;23:1-7</a> | en_US |
| dc.identifier.uri | https://hdl.handle.net/10037/12840 | |
| dc.language.iso | eng | en_US |
| dc.publisher | UiT The Arctic University of Norway | en_US |
| dc.publisher | UiT Norges arktiske universitet | en_US |
| dc.rights.accessRights | openAccess | en_US |
| dc.rights.holder | Copyright 2018 The Author(s) | |
| dc.subject.courseID | DOKTOR-003 | |
| dc.subject | VDP::Medisinske Fag: 700::Klinisk medisinske fag: 750::Nevrokirurgi: 786 | en_US |
| dc.subject | VDP::Medical disciplines: 700::Clinical medical disciplines: 750::Neurosurgery: 786 | en_US |
| dc.title | Perioperative quality assurance in neurosurgery | en_US |
| dc.type | Doctoral thesis | en_US |
| dc.type | Doktorgradsavhandling | en_US |


 English
English norsk
norsk